DD 2870 Template
DD 2870 Template
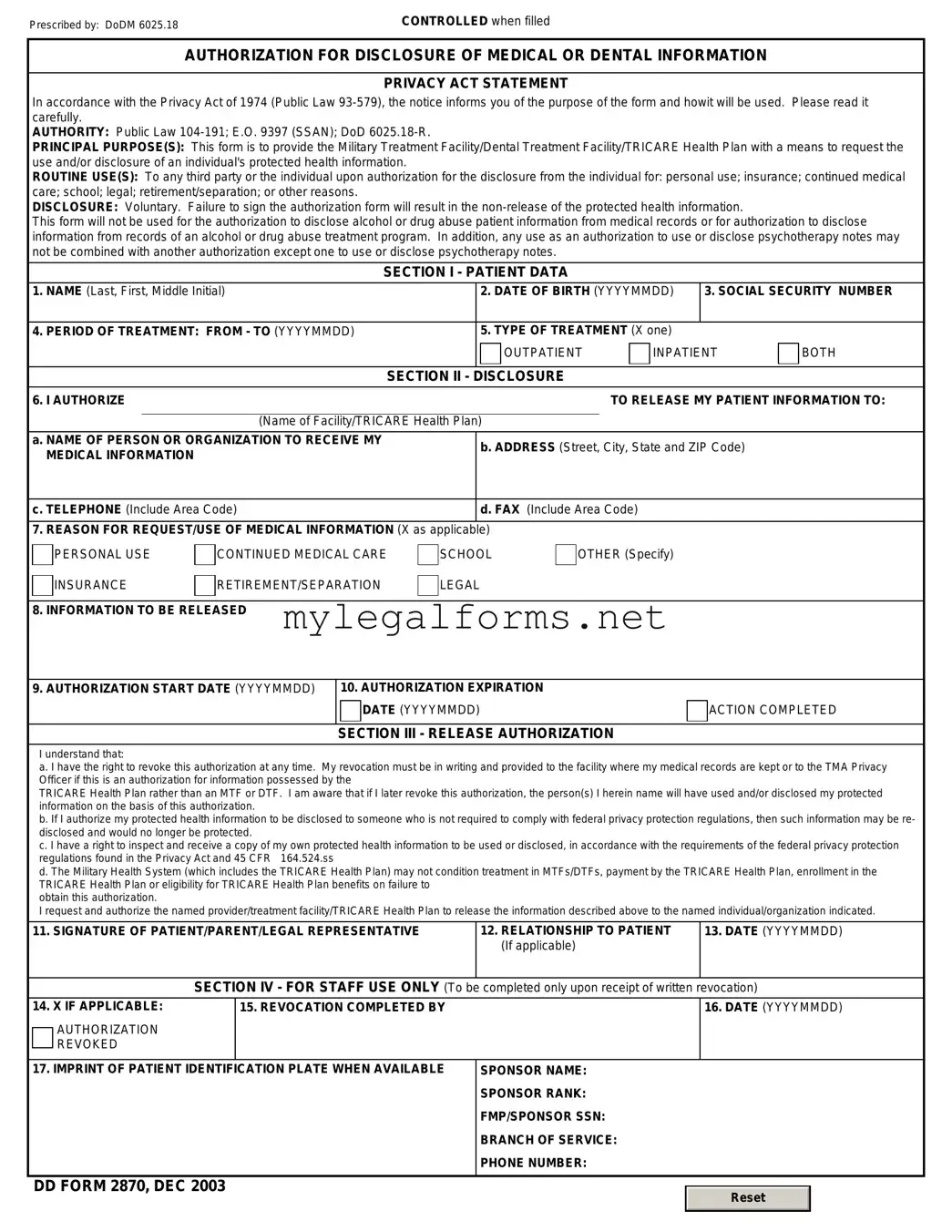
The DD 2870 form is an essential document for service members and their families, providing a streamlined process for requesting medical care and benefits. This form plays a critical role in ensuring that individuals receive the necessary support during their service and after transitioning to civilian life. It captures vital information, including personal details, eligibility for benefits, and specific medical needs. By completing the DD 2870, service members can facilitate access to healthcare services, ensuring timely treatment and support. The form also aids in the documentation of medical history, which can be crucial for future care. Understanding how to properly fill out this form is important for all eligible personnel, as it directly impacts their access to vital resources and benefits.
The DD 2870 form is essential for individuals seeking to authorize the release of their medical records. Here are key takeaways regarding its use:
Understanding these points can help streamline the process of obtaining important medical records.
Corporate Stock Ledger Example - The stockholder's name is required to specify the individual involved in the transaction.
The California Notice to Quit form is a legal document used by landlords to formally notify tenants of their intent to terminate a rental agreement. This notice serves as a crucial step in the eviction process, allowing tenants to understand the reasons for their eviction and the time frame in which they must vacate the premises. For more information on this important legal tool, you can visit californiadocsonline.com/notice-to-quit-form, as understanding this form is essential for both landlords and tenants to navigate their rights and responsibilities effectively.
International Driver License Aaa - By applying for an IDP, you enhance your travel convenience and confidence.
Ccorp - S corporations must adhere to specific operational guidelines post-election on Form 2553.
The DD 2870 form is a crucial document used in the military context, particularly for requesting access to personal health information. However, it is often accompanied by other forms and documents that facilitate various processes related to health care and benefits. Below is a list of five documents that are commonly used alongside the DD 2870 form.
Understanding these documents and their purposes is essential for service members and veterans navigating the complexities of health care and benefits. Each form plays a distinct role in ensuring that individuals receive the support and services they are entitled to based on their military service.
When filling out the DD 2870 form, it's important to follow certain guidelines to ensure accuracy and compliance. Here’s a helpful list of dos and don’ts to keep in mind:
The DD 2870 form, also known as the "Authorization for Disclosure of Medical or Dental Information," is crucial for service members and their families when seeking medical care. However, errors during the completion of this form can lead to delays or denials of services. Understanding common mistakes can help ensure that the form is filled out correctly.
One frequent mistake is incomplete information. Individuals often neglect to fill in all required fields, such as personal identification details or specific medical information. Omitting these details can result in processing delays, as the reviewing authority may need to request the missing information before proceeding.
Another common error involves incorrect signatures. Signatures must match the name provided on the form. If a spouse or other family member signs on behalf of the service member without proper authorization, it may invalidate the form. Ensuring that the correct individual signs is essential for the form's acceptance.
Many people also overlook the date on the form. Failing to date the authorization can lead to questions about the form's validity. Proper dating helps clarify the timeline of consent and ensures that the authorization remains relevant.
In addition, individuals sometimes select the wrong purpose for the disclosure. The form allows for various purposes, such as treatment or legal proceedings. Choosing the incorrect purpose can complicate the process, as the reviewing authority may not understand the context of the request.
Some applicants fail to review the privacy notice included with the form. This notice outlines how the information will be used and shared. Ignoring this section can lead to misunderstandings regarding privacy rights and the extent of information sharing.
Another mistake involves not providing contact information for the individual or organization requesting the disclosure. Without this information, the healthcare provider may struggle to fulfill the request efficiently. Including accurate contact details is vital for a smooth communication process.
Additionally, individuals may not keep a copy of the completed form for their records. Retaining a copy can be invaluable for future reference, especially if questions arise regarding the authorization or if the form needs to be resubmitted.
Lastly, individuals sometimes submit the form to the wrong office. Each military branch has specific protocols for handling medical information requests. Ensuring that the form is sent to the correct office can prevent unnecessary delays in processing.
By being aware of these common mistakes, individuals can improve their chances of successfully completing the DD 2870 form and receiving the medical care they need without unnecessary complications.
| Fact Name | Description |
|---|---|
| Purpose | The DD 2870 form is used to authorize the release of medical information. |
| Who Uses It? | This form is primarily used by military personnel and their dependents. |
| Submission Process | Once completed, the form must be submitted to the appropriate medical facility. |
| Privacy Compliance | The form complies with HIPAA regulations to protect personal health information. |
| Expiration | Authorization granted through the DD 2870 typically expires after one year. |
| State-Specific Laws | In California, the form is governed by the Confidentiality of Medical Information Act. |
| Signature Requirement | A valid signature from the patient or their legal representative is mandatory. |
Prescribed by: DoDM 6025.18 |
CONTROLLED when filled |
AUTHORIZATION FOR DISCLOSURE OF MEDICAL OR DENTAL INFORMATION
PRIVACY ACT STATEMENT
In accordance with the Privacy Act of 1974 (Public Law
AUTHORITY: Public Law
PRINCIPAL PURPOSE(S): This form is to provide the Military Treatment Facility/Dental Treatment Facility/TRICARE Health Plan with a means to request the use and/or disclosure of an individual's protected health information.
ROUTINE USE(S): To any third party or the individual upon authorization for the disclosure from the individual for: personal use; insurance; continued medical care; school; legal; retirement/separation; or other reasons.
DISCLOSURE: Voluntary. Failure to sign the authorization form will result in the
This form will not be used for the authorization to disclose alcohol or drug abuse patient information from medical records or for authorization to disclose information from records of an alcohol or drug abuse treatment program. In addition, any use as an authorization to use or disclose psychotherapy notes may not be combined with another authorization except one to use or disclose psychotherapy notes.
SECTION I - PATIENT DATA
1. NAME (Last, First, Middle Initial) |
|
2. DATE OF BIRTH (YYYYMMDD) |
3. SOCIAL SECURITY NUMBER |
|||
|
|
|
|
|
|
|
4. PERIOD OF TREATMENT: FROM - TO (YYYYMMDD) |
|
5. TYPE OF TREATMENT (X one) |
|
|
||
|
|
|
OUTPATIENT |
INPATIENT |
BOTH |
|
|
|
|
|
|
|
|
|
|
SECTION II - |
DISCLOSURE |
|
|
|
6. I AUTHORIZE |
|
|
TO RELEASE MY PATIENT INFORMATION TO: |
|||
|
|
|
|
|
||
|
(Name of Facility/TRICARE Health Plan) |
|
|
|
||
a. NAME OF PERSON OR ORGANIZATION TO RECEIVE MY |
|
b. ADDRESS (Street, City, State and ZIP Code) |
|
|||
MEDICAL INFORMATION |
|
|
||||
|
|
|
|
|
||
|
|
|
|
|
||
c. TELEPHONE (Include Area Code) |
|
d. FAX (Include Area Code) |
|
|
||
|
|
|
|
|
||
7. REASON FOR REQUEST/USE OF MEDICAL INFORMATION (X as applicable) |
|
|
|
|
||
PERSONAL USE
INSURANCE
CONTINUED MEDICAL CARE
RETIREMENT/SEPARATION
SCHOOL
LEGAL
OTHER (Specify)
8. INFORMATION TO BE RELEASED
9. AUTHORIZATION START DATE (YYYYMMDD)
10. AUTHORIZATION EXPIRATION
DATE (YYYYMMDD)
SECTION III - RELEASE AUTHORIZATION
ACTION COMPLETED
I understand that:
a. I have the right to revoke this authorization at any time. My revocation must be in writing and provided to the facility where my medical records are kept or to the TMA Privacy Officer if this is an authorization for information possessed by the
TRICARE Health Plan rather than an MTF or DTF. I am aware that if I later revoke this authorization, the person(s) I herein name will have used and/or disclosed my protected information on the basis of this authorization.
b. If I authorize my protected health information to be disclosed to someone who is not required to comply with federal privacy protection regulations, then such information may be re- disclosed and would no longer be protected.
c. I have a right to inspect and receive a copy of my own protected health information to be used or disclosed, in accordance with the requirements of the federal privacy protection regulations found in the Privacy Act and 45 CFR 164.524.ss
d. The Military Health System (which includes the TRICARE Health Plan) may not condition treatment in MTFs/DTFs, payment by the TRICARE Health Plan, enrollment in the TRICARE Health Plan or eligibility for TRICARE Health Plan benefits on failure to
obtain this authorization.
I request and authorize the named provider/treatment facility/TRICARE Health Plan to release the information described above to the named individual/organization indicated.
11. SIGNATURE OF PATIENT/PARENT/LEGAL REPRESENTATIVE |
12. RELATIONSHIP TO PATIENT |
13. DATE (YYYYMMDD) |
|
(If applicable) |
|
|
|
|
SECTION IV - FOR STAFF USE ONLY (To be |
completed only upon receipt of written revocation) |
|
14. X IF APPLICABLE:
AUTHORIZATION REVOKED
15. REVOCATION COMPLETED BY
16.DATE (YYYYMMDD)
17. IMPRINT OF PATIENT IDENTIFICATION PLATE WHEN AVAILABLE |
SPONSOR NAME: |
||
|
SPONSOR RANK: |
||
|
FMP/SPONSOR SSN: |
||
|
BRANCH OF SERVICE: |
||
|
PHONE NUMBER: |
||
|
|
|
|
DD FORM 2870, DEC 2003 |
|
|
|
|
Reset |
|
|
|
|
|
|
|
|
|
|