Medication Error Template
Medication Error Template
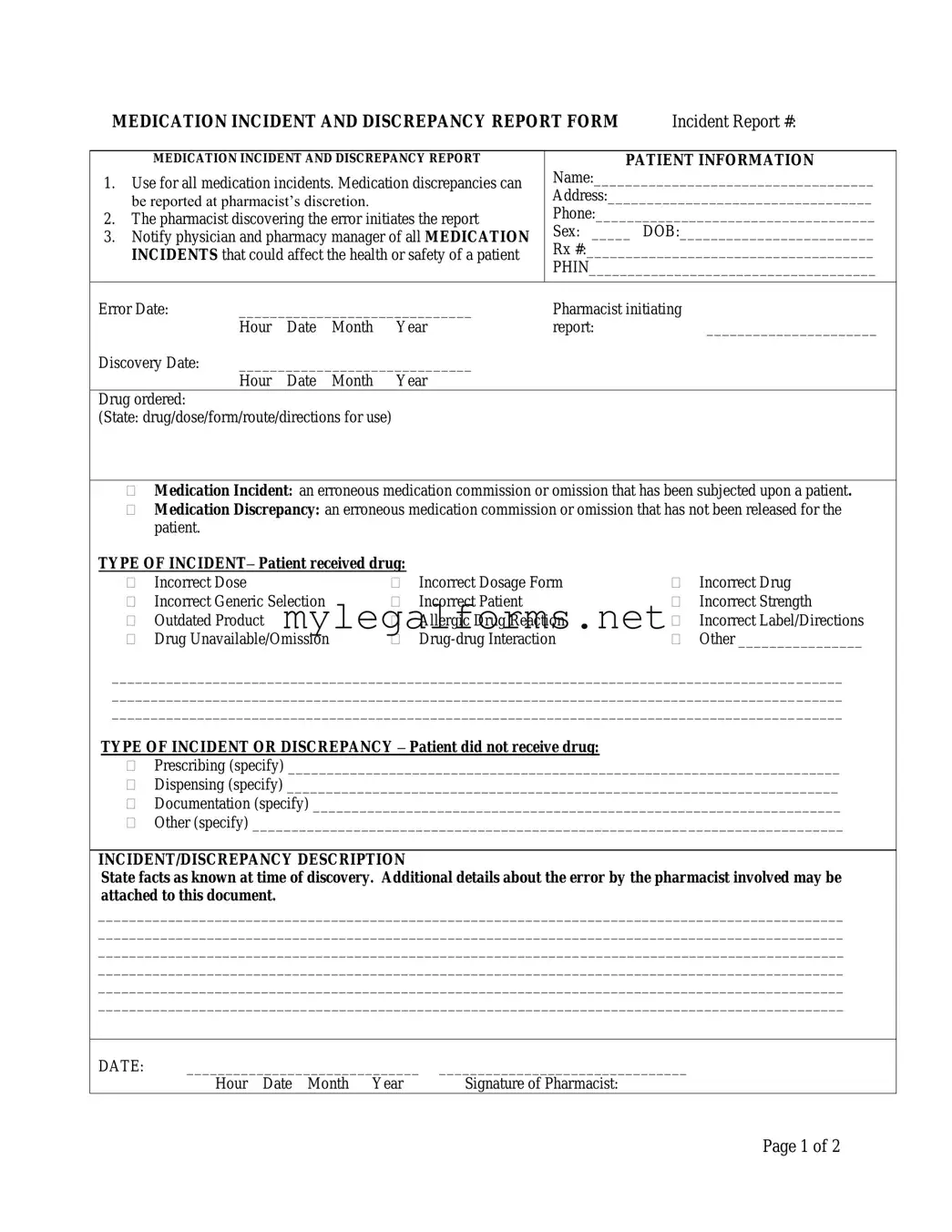
Medication errors can have serious consequences for patient safety and well-being, making it essential for healthcare providers to have a structured process for reporting and addressing these incidents. The Medication Incident and Discrepancy Report Form serves as a critical tool in this regard, allowing pharmacists to document errors and discrepancies in medication administration. This form is initiated by the pharmacist who discovers the error and is designed to capture vital information such as patient details, the nature of the incident, and the severity of the error. It includes sections for identifying the type of medication involved, whether the patient received the wrong drug or dosage, and any contributing factors that may have led to the mistake. Additionally, it outlines the necessary notifications to be made to physicians and pharmacy managers, ensuring that all relevant parties are informed. By systematically documenting these incidents, the form not only aids in immediate response and resolution but also contributes to long-term improvements in medication safety practices.
Filling out and utilizing the Medication Error form is essential for maintaining patient safety and improving pharmacy practices. Here are six key takeaways regarding the process:
Roof Guarantee - Homebuyers can take comfort in knowing the roof has a quality warranty.
The process of homeschooling requires parents to fulfill certain legal obligations, and an essential component of this is the submission of the California Homeschool Letter of Intent form. This document officially declares a family's intention to educate their children at home, and it is crucial for ensuring compliance with state regulations. For detailed guidance on completing this form, parents can refer to resources available at californiadocsonline.com/homeschool-letter-of-intent-form/, which can assist them in navigating this important step in the homeschooling journey.
Free Insurance Card Template - Make sure all fields are properly filled to ensure compliance with state laws.
When a medication error occurs, it’s crucial to have a comprehensive set of documents to ensure proper reporting, analysis, and resolution. Each of these documents plays a vital role in the overall medication safety process. Below is a list of forms and documents commonly used alongside the Medication Error form.
These documents collectively contribute to a robust framework for managing medication errors. They not only help in addressing individual incidents but also play a crucial role in fostering a culture of safety and continuous improvement within healthcare settings.
When filling out the Medication Error form, it is crucial to follow specific guidelines to ensure accuracy and clarity. Here’s a list of what to do and what to avoid.
When filling out the Medication Error form, individuals often make several common mistakes that can lead to confusion or incomplete information. One frequent error is failing to provide complete patient information. This includes not filling in the patient's name, address, phone number, sex, or date of birth. Omitting any of these details can hinder proper follow-up and tracking of the incident.
Another mistake is not clearly stating the type of incident. The form includes various categories for medication errors, such as incorrect dose or incorrect drug. If the individual does not specify the type of incident accurately, it can complicate the investigation process and lead to misunderstandings about the nature of the error.
Some people also neglect to describe the incident or discrepancy in detail. Providing a thorough account of what happened is crucial for understanding the context of the error. Vague descriptions can leave out important information that may be necessary for addressing the issue effectively.
Additionally, not notifying the physician or pharmacy manager as required can be a significant oversight. The form emphasizes the importance of notifying these parties about incidents that could affect patient health or safety. Failure to do so can lead to a lack of necessary medical intervention or oversight.
Another common error involves inaccurate completion of the contributing factors section. This section requires the pharmacist to identify what led to the error. If this part is filled out incorrectly or not at all, it can prevent the pharmacy from implementing necessary changes to prevent future incidents.
Individuals may also forget to sign and date the form properly. Both the pharmacist and the pharmacy manager need to provide their signatures and dates. Missing signatures can delay the process and create confusion about who was responsible for the report.
Some people may not check the severity of the incident accurately. It is important to assess the impact of the error on the patient’s condition. Misclassifying the severity can lead to inappropriate responses or follow-up actions.
Lastly, not following up on the resolution of the problem can be a significant mistake. The form includes a section for documenting how the issue will be resolved. If this section is left blank or inadequately completed, it may result in unresolved issues that could lead to further errors in the future.
| Fact Name | Description |
|---|---|
| Purpose of the Form | This form is used to report all medication incidents and discrepancies, ensuring patient safety and proper documentation. |
| Initiation of Report | The pharmacist who discovers the medication error is responsible for initiating the report. |
| Notification Requirements | All medication incidents that could impact a patient’s health or safety must be reported to both the physician and the pharmacy manager. |
| Types of Incidents | Various types of medication incidents can be reported, including incorrect dose, incorrect drug, and allergic reactions, among others. |
| Patient Information | The form requires detailed patient information, including name, address, phone number, and date of birth for accurate record-keeping. |
| Contributing Factors | Pharmacists must identify contributing factors to the error, such as improper patient identification or misinterpretation of drug orders. |
| State-Specific Regulations | Different states may have specific laws governing medication error reporting, such as the California Business and Professions Code Section 4160. |
MEDICATION INCIDENT AND DISCREPANCY REPORT FORM |
Incident Report #: |
MEDICATION INCIDENT AND DISCREPANCY REPORT
1.Use for all medication incidents. Medication discrepancies can be reported at pharmacist’s discretion.
2.The pharmacist discovering the error initiates the report
3.Notify physician and pharmacy manager of all MEDICATION INCIDENTS that could affect the health or safety of a patient
PATIENT INFORMATION
Name:____________________________________
Address:__________________________________
Phone:____________________________________
Sex: _____ DOB:_________________________
Rx #:_____________________________________
PHIN_____________________________________
Error Date: |
______________________________ |
Pharmacist initiating |
|
|||
|
Hour |
Date |
Month |
Year |
report: |
______________________ |
Discovery Date: |
______________________________ |
|
|
|||
|
Hour |
Date |
Month |
Year |
|
|
Drug ordered: |
|
|
|
|
|
|
(State: drug/dose/form/route/directions for use) |
|
|
|
|||
Medication Incident: an erroneous medication commission or omission that has been subjected upon a patient.
Medication Discrepancy: an erroneous medication commission or omission that has not been released for the patient.
TYPE OF INCIDENT– Patient received drug: |
|
|
|
||
|
Incorrect Dose |
|
Incorrect Dosage Form |
|
Incorrect Drug |
|
Incorrect Generic Selection |
|
Incorrect Patient |
|
Incorrect Strength |
|
Outdated Product |
|
Allergic Drug Reaction |
|
Incorrect Label/Directions |
|
Drug Unavailable/Omission |
|
|
Other ________________ |
|
______________________________________________________________________________________________
______________________________________________________________________________________________
______________________________________________________________________________________________
TYPE OF INCIDENT OR DISCREPANCY – Patient did not receive drug:
Prescribing (specify) _______________________________________________________________________
Dispensing (specify) _______________________________________________________________________
Documentation (specify) ____________________________________________________________________
Other (specify) ____________________________________________________________________________
INCIDENT/DISCREPANCY DESCRIPTION
State facts as known at time of discovery. Additional details about the error by the pharmacist involved may be attached to this document.
________________________________________________________________________________________________
________________________________________________________________________________________________
________________________________________________________________________________________________
________________________________________________________________________________________________
________________________________________________________________________________________________
________________________________________________________________________________________________
DATE: |
______________________________ |
________________________________ |
|
Hour Date Month Year |
Signature of Pharmacist: |
Page 1 of 2
CONTRIBUTING FACTORS
(To be completed by pharmacist responsible)
|
Improper patient identification |
Misread/misinterpreted drug order (include verbal orders) |
|
|
Incorrect transcription |
|
Drug unavailable |
Lack of patient counselling |
|
Other |
|
|
DATE: |
______________________________ |
__________________ |
|
|
||||
|
|
Hour Date Month Year |
Signature |
|
|
|
|||
|
NOTIFICATION – Complete the following information according to Standards of Practice. |
||||||||
1. |
Patient notified: |
|
|
|
|
|
|
|
|
|
|
|
___________________________ |
|
|||||
|
|
|
Hour |
Date |
Month |
Year |
|||
2. |
Physician notified: ____ |
______________________________ |
|
||||||
|
|
Yes/No |
Hour |
Date |
Month |
Year |
|||
|
|
|
|
|
|
|
|
|
|
|
SEVERITY |
|
|
|
|
|
|
|
|
|
|
None |
|
No change in patient’s condition: no medical intervention |
|||||
|
|
Minor |
|
|
|
required |
|
|
|
|
|
Major |
|
Produces a temporary systemic or localized response: does |
|||||
|
|
|
|
|
|
not cause ongoing complications |
|||
|
|
|
|
Requires immediate medical intervention |
|||||
|
OUTCOME OF INVESTIGATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Problem Identification |
|
|
|
Action |
|
|
|
|
|
|
Lack of knowledge |
|
|
Education provided |
||||
|
|
Performance problem |
|
|
Policy/procedure changed |
||||
|
|
Administration problem |
|
|
System changed |
|
|
||
|
|
Other |
|
|
Individual awareness |
||||
|
|
|
|
|
Group awareness |
||||
|
|
|
|
|
Other |
|
|
|
|
|
|
|
|
|
|||||
|
RESOLUTION OF PROBLEM THAT RESULTED IN THE ERROR BEING MADE: |
||||||||
|
|
|
|
|
|
|
|
||
|
Signature: |
Date: |
Signature: |
Date: |
|||||
|
(Pharmacist filling out the form) |
|
|
|
(Pharmacy Manager) |
||||
PHARMACY USE ONLY
Page 2 of 2